



TUG flap (Transverse Upper Gracilis Flap)
What is TUG flap?
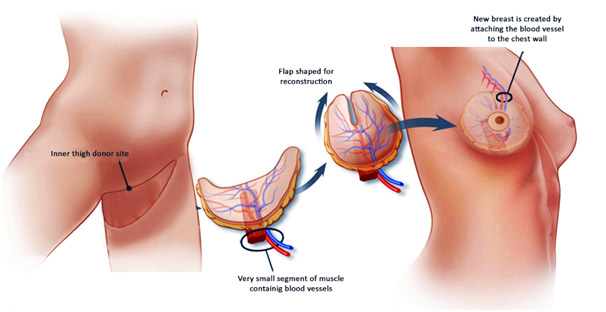
- The skin and fat along the upper inner thigh is taken along with gracilis muscle and it’s blood supply to constitute the Transverse Upper Gracilis (TUG) Flap. This flap is widely used for breast reconstruction.Gracilis is one of the many muscles in the inner thigh which is responsible for bringing the thigh towards the centre. As many muscles in the thigh can do the same action, taking this muscle leaves no functional problems. The skin and fat look like a “ melon slice” which can be made into a cone shape to form a soft and shapely breast. The peak of the cone becomes the nipple. The blood vessel accompanying the flap is then connected to the blood vessel in the chest by advanced microsurgery to form a nice breast of a good shape.
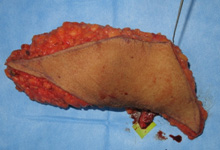
The TUG flap from the inner thigh is shaped like a breast by folding it
Primary nipple reconstruction is done

- For a patient who had breast cancer both sides, the breasts were removed both sides ,TUG flaps along with primary nipple reconstruction was done on both sides to make it look like breasts

- The final result after TUG flap reconstruction for both sides of the breast