



How common is oral cancer?
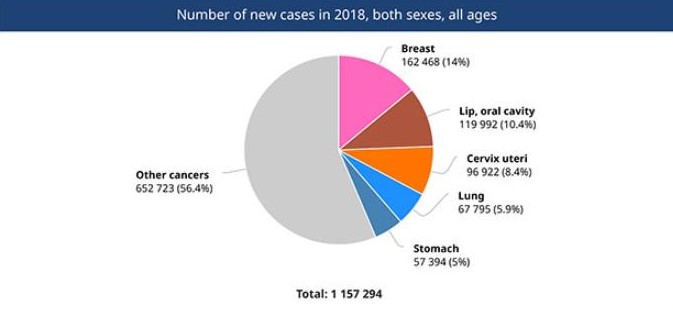
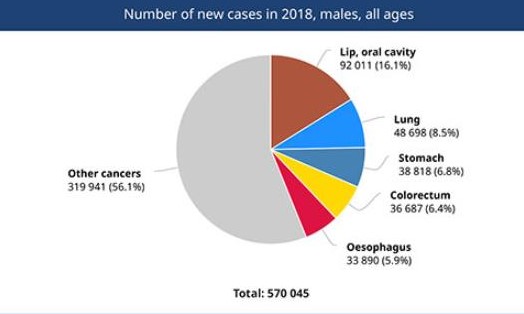
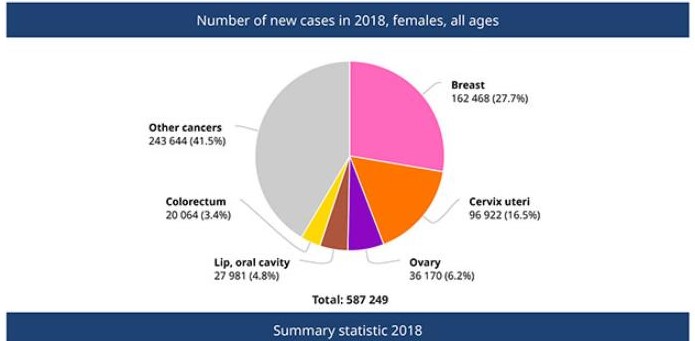
- Oral cancer is very common. Oral cancers are the second leading cause of cancer in India after breast cancer. Around one-third of oral cancer cases in the world is present in India. Oral cancer is the most common cancer in men. It accounts for 16% of all cancers in men and 10% of all cancers in both men and women in India.
Reconstruction of the tumours
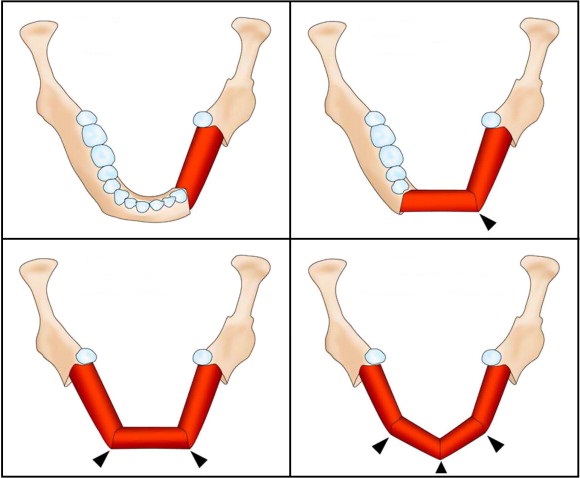
- After removing the tumour with a wide margin, there can be a significant defect that needs to be covered and reconstructed. Reconstruction helps to give form and symmetry to the face. The recent advances in technology have allowed us to use 3D printing technology to contour the new bone the same way as the native bone to attain facial symmetry giving a much superior cosmetic outcome.
What is the need for reconstruction after removal of oral cancer?
- Good reconstruction of the defects is essential to provide good outcomes in speech, eating, swallowing, and providing good symmetry to the face. Good reconstruction after oral cancer helps to improve the quality of life of the patient massively.
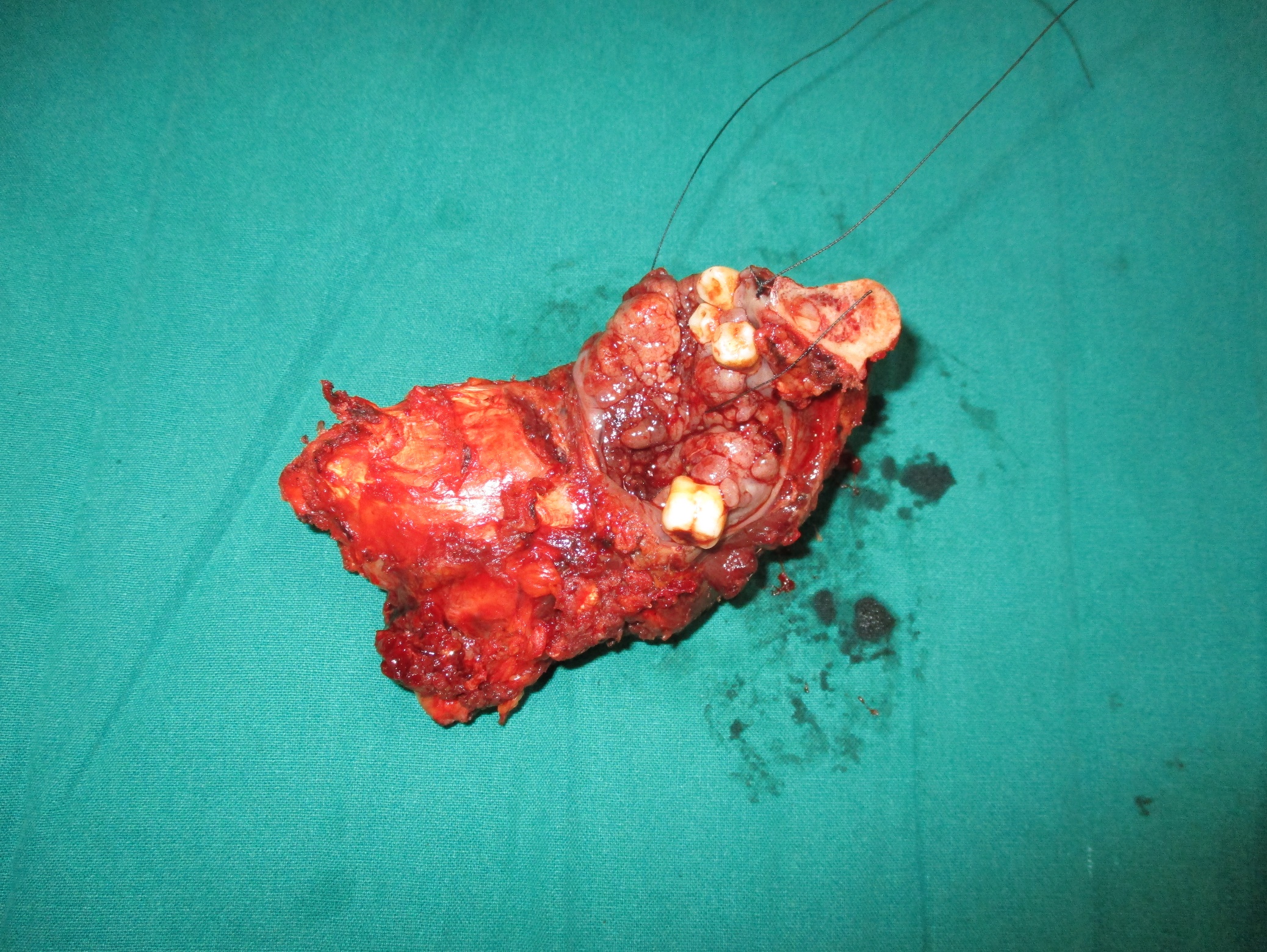
- After excision of the tumour, the tissues need to be closed and sutured back. The ability to reconstruct the defect after oral cancer surgery well gives the surgeon the confidence to excise the cancer with good margins. This will help improve the survival of the patient.
- Patients reconstructed well after oral cancer surgery look better than patients who have not been reconstructed.
- Thus reconstruction after oral cancer surgery becomes an integral part of cancer surgery and treatment.




How do we reconstruct after surgical removal of tumour?
Local flap reconstruction
- Local flap reconstruction involves replacing the defect with tissue from the adjacent area to cover the defect. Local flap reconstruction suits best when the defects are small, and there is sufficient tissue surrounding the area to cover and fill up the defect. If the defect is large and there is insufficient tissue to cover the defect, microvascular free flaps are more suitable.
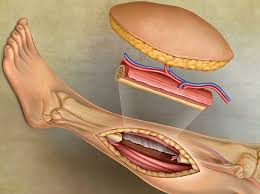
Microvascular free flap reconstruction.
- Microvascular free flap reconstruction remains the gold standard for reconstruction because it helps us provide adequate tissue for reconstruction, provide tissues such as bone, fat, and skin, improve the functional outcome, and maintain symmetry of the face. It also helps us to reduce the morbidity of the donor site.


Facts at a glance about surgery and post-operative instructions: ( May vary from person to person)
| Type of anaesthesia | General Anaesthesia |
|---|---|
| Surgery time | 2 - 6 hours |
| Hospital stay | 3 - 10 days |
| Mobilisation | 2nd day |
| Suture removal | 12th day |
| Self-care | 1-2 weeks |
| Full recovery | 4- 6 weeks |
| Return to work | 4 weeks |