What is Early Breast Cancer?
How are non palpable breast cancers diagnosed?
How are palpable breast cancers diagnosed?
What investigations are done for Early Breast Cancer?
How is Early Breast Cancer treated?
What are the surgical modalities for treating Early Breast Cancer?
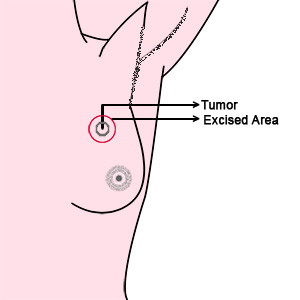
Breast Conservative Therapy
- This can be done only for a small tumour in a large breast wherein we remove the breast cancer along with a small margin of tissue. If there are multiple lesions in the breast this procedure can not be done.The patient would definitely need radiotherapy after this procedure. By doing this we can conserve the breasts.
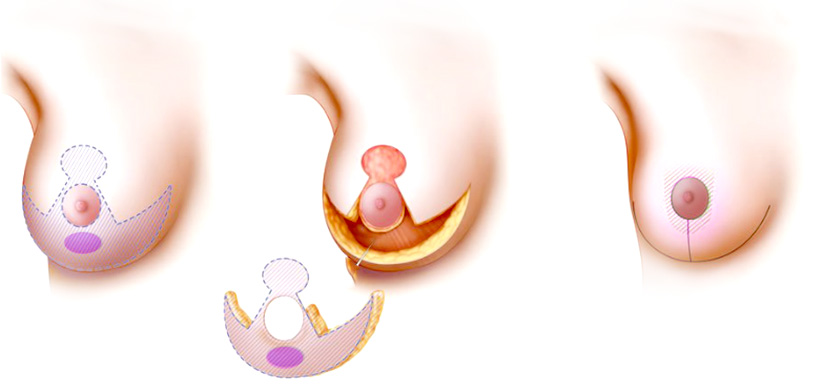
Therapeutic Mammaplasty
- This procedure is done for slightly larger tumours in a large breast where in we remove a part of the breast and use breast reduction plastic surgical techniques to reduce the size of the breast. This breast would definitely need radiotherapy after the procedure.
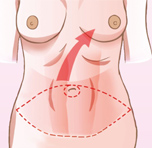
Mastectomy with Reconstruction
- Here the whole breast is removed. This is done for small breasts, multiple tumours in the breast and breast cancers which present in an advanced stage. We offer the full gamut of reconstruction possibilities for the patient. The best method of reconstruction would be autologous reconstruction where we take the patients own tissues such as the tummy, inner thighs, back or buttocks to make a new breast. Reconstruction of the breast is best done at the same time of the mastectomy or removal of the breast as the patient wakes up with a new breast, surgery is done in one operation and the cosmetic result of a breast done at the same time of removal of the breast is better than when reconstructed at a later date.
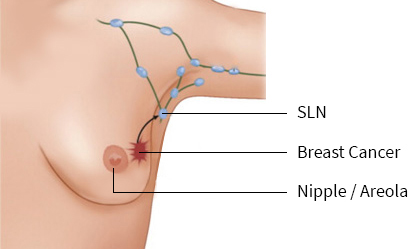
Sentinel Lymph node Biopsy
- Sentinel lymph node is the first lymph node that drains the breast cancer. It is assumed that if this lymph node is biopsied and no tumour is found then more radical procedures such a axillary lymph node dissection can be avoided. However if tumour is found in the lymph node biopsied, a complete axillary lymph node dissection needs to be done.
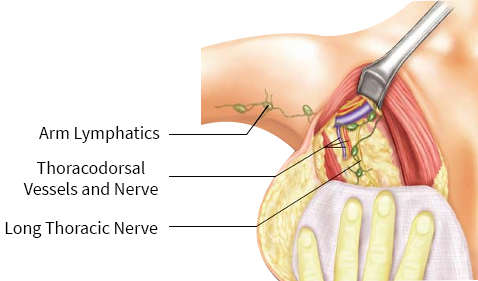
Axillary Lymph Node Dissection
- Axillary lymph node dissection is done when there is a lymph node which is palpable in the axilla or if sentinel lymph node biopsy is positive. Here the entire group of lymphatics in the axilla is removed.